Guest Post by Mark A. Largent
Medical advice—long under the authority of doctors and public health officials—is now freely available on the Internet, and nowhere are the effects of this trend more visible than around the issue of vaccines. The web provides easy access to the kinds of criticism of vaccines that was once available only from fringe natural-health booksellers and alternative medical providers. In an effort to counter these claims, mainstream healthcare providers offer orthodox scientific and medical information to consumers on the Internet. The result is a set of competing claims online that are nearly impossible for parents to reconcile into a coherent plan for vaccinating their children.
Reports of two court cases have recently emerged online that powerfully demonstrate how readers on either side of the debates over the safety of vaccines are armed with evidence to support wildly divergent views. Among mainstream medical providers, the widespread consensus is that there is no causal link between vaccines and autism. However, over the last several weeks, news has circulated on alternative medical sites about two federal court decisions that “confirmed … that there is a link between the MMR [measles, mumps, and rubella] vaccine, autism, and stomach disorders.” Citing court records, news reports (which have also been published in mainstream sources like the Huffington Post) purport to show “repeated admissions by drug companies and government alike that vaccines do in fact cause autism.”
Here are the facts of the cases: The federal court that hears cases of people allegedly injury by vaccines has recently decided in favor of the parents of two children who say that their children developed symptoms of autism because of the adverse side effects of vaccines. The so-called “vaccine court,” which was established by the 1986 National Childhood Vaccine Injury Act, is charged with resolving vaccine injury claims and provides compensation from a trust fund that is financed by a 75 cent excise tax on every vaccine. Vaccine manufactures are protected from lawsuits because the vaccine court hears claims and pays injured parties from the trust without ever assigning fault. The court typically pays out between $100 and $200 million per year.
In the first case, the court decided that a 10-year-old boy from California named Ryan Mojabi suffered a “severe and debilitating injury to his brain, described as Autism Spectrum Disorder” that was caused by brain swelling that occurred after he had been vaccinated with MMR. As a result, Ryan now suffers from the symptoms associated with autism. He was awarded an undisclosed amount that could total $10 million or more.
In a second case, which had been in and out of court for nearly a decade, 15-month-old Emily Moller had developed a high fever and seizures after being vaccinated with the combined vaccine against diphtheria, pertussis, and tetanus. She has been diagnosed on the autism spectrum. Late last year the case was settled, and Emily will receive an estimated $9 million in compensation.
These cases provide a tremendously powerful rhetorical weapon to those who claim that vaccines can cause autism. Reports of the cases are circulating widely on the web, and they add fuel to the online debates that confront new parents as they seek out information on vaccines. Both children had suffered from rare but documented adverse side effects from being vaccinated, and in both cases serious long-term damages are evident. It is doubtlessly unfortunate that these children were injured in the course of receiving routine vaccines, but cases like theirs are very rare, and vaccines safely protect the vast majority of children against diseases that once caused considerable death, injury, and discomfort.
How, then, did we end up in a situation where incredibly uncommon cases like Ryan’s or Emily’s have so much rhetorical power? And, what are we to make of these two cases? The problem, I submit, does not reside in the vaccines themselves, but in the fact that we have failed to have honest conversations about difficult issues related to vaccines.
Today’s concerns about vaccines can be traced to allegations that emerged in the late 1990s of a link between vaccines and autism. In Britain, a preliminary report by a research team suggested that the MMR vaccine might sometimes damage children’s digestive tracts, which in turn might lead to developmental disorders associated with autism. At about the same time, as part of an overhaul of the Food and Drug Administrative, reports emerged that a mercury-laden preservative—Thimerosal—had long been used in childhood vaccines. The symptoms of mercury poisoning share many similarities with autism and public health authorities had long warned parents of the dangers of heavy metals like mercury and lead, so parents were shocked to learn that their children had been injected with vaccines that contained mercury.
Both of the scientific controversies that alleged an association between vaccines and autism were resolved by 2004. Today, the consensus of the scientific and medical communities is that neither the MMR vaccine nor Thimerosal is responsible for the recent rapid increase in the diagnoses of autism. Instead, most authorities point to increasing awareness, relaxed diagnostic criteria, and a number of social and economic incentives for diagnoses to explain the increasing rate of diagnoses.
While the scientific controversy over the alleged link between vaccines and autism has been resolved for almost a decade now, the political controversy has continued to rage. Advocates of the claim that vaccines cause or trigger the symptoms associated with autism have developed an alternative set of news sources to provide evidence to those who believe that vaccines are unsafe and that the government and mainstream media are covering up the evidence. As the potentially complicated discussions about the merits and potential problems of the modern vaccine schedule have become confined almost entirely to the vaccines-cause-autism debate, advocates on either side of the issue promulgate irreconcilable claims.
In my 2012 book Vaccine: The Debate in Modern America, I argue that the rapid increase in the size of the vaccine schedule and Americans’ increasing concerns about vaccines were not merely coincidental. Under today’s vaccine schedule a fully vaccinated 6-year old will have received about three dozen inoculations of over 50 vaccines, most of them in the first 18 months of life. This has motivated considerable concern among parents about unintended side effects of vaccines. About 40% of American parents report that they have intentionally refused or delayed a recommended vaccine for their children, and about 1 in 8 parents have refused a state-mandated vaccine. Safety concerns about new vaccines and a widespread belief that we give too many vaccines, too early, against too many diseases are at the root of many parents’ concerns. Vaccine-anxious is the term I used for people who expressed concerns like these while generally accepting that vaccines are usually safe and effective. Elsewhere, I have argued that we ought to be very careful about mistakenly labeling vaccine-anxious people as anti-vaccinators. In terms of maintaining high levels of vaccine compliance, they are effectively “swing-voters,” and it is vital that we keep them within the fold. By mislabeling them as anti-vaccinators, we push them into the arms of those who have amassed ample evidence to support their fears about unintended side effects from vaccines.
Concerns that vaccines might cause autism are actually a proxy for a much more complex set of concerns, which I describe in the book. Some of these are practical, like how we cram as many as six vaccinations into one office visit. Others are moral, because half of childhood vaccines were researched and produced with the use of cells derived from aborted fetuses. Still others are deeply philosophical, including concerns that we have entered a realm of medical enhancements that fundamentally alter human beings. The vaccines-cause-autism proxy debate allows us to avoid actually engaging these complicated topics. It also allows many different views to gather under a single set of claims, which explains why criticisms of vaccines are launched by voices from every corner of the political spectrum.
The two cases from the vaccine court that have generated so much discussion among opponents of the modern vaccine schedule are influential only because we have failed to engage the real issues that animate the vaccines-cause-autism proxy debate. Until we do, the large and active community of people who express serious concerns about vaccines will continue amass evidence that will adversely affect the decisions of millions of vaccine-anxious parents.
 Mark A. Largent is a historian of science and medicine and an Associate Dean and Associate Professor at Michigan State University. His teaching and research focus on the role of scientists and physicians in public policy debates. His most recent book, Vaccine: The Debate in Modern America (Johns Hopkins, 2012) analyzes the vaccine-autism debate and contemporary concerns about the modern vaccination schedule. He is currently completing a book on the history of Reye’s syndrome.
Mark A. Largent is a historian of science and medicine and an Associate Dean and Associate Professor at Michigan State University. His teaching and research focus on the role of scientists and physicians in public policy debates. His most recent book, Vaccine: The Debate in Modern America (Johns Hopkins, 2012) analyzes the vaccine-autism debate and contemporary concerns about the modern vaccination schedule. He is currently completing a book on the history of Reye’s syndrome.
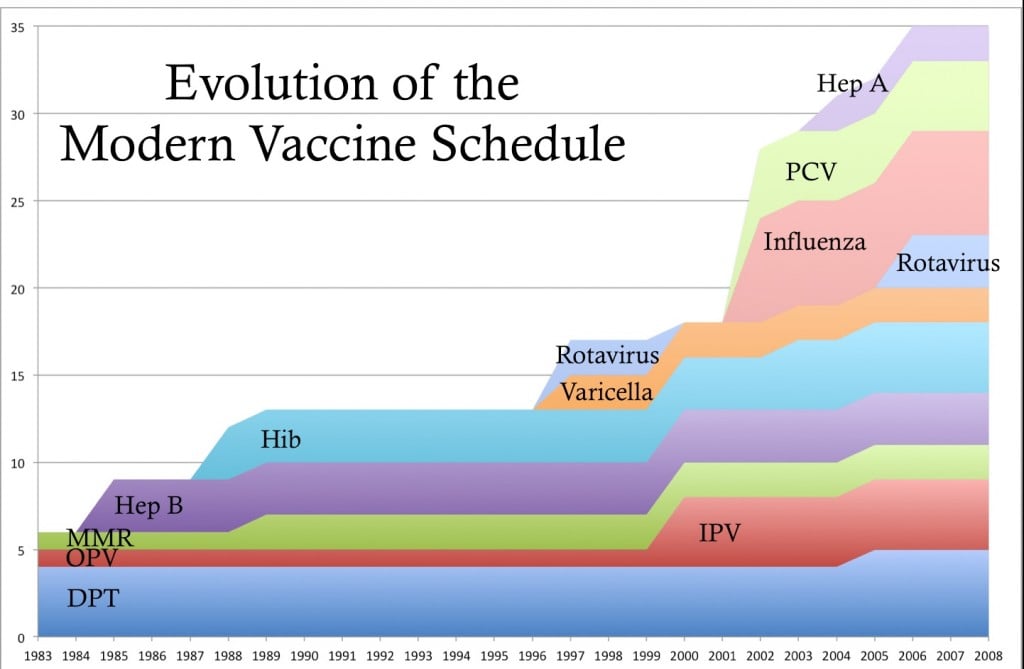
What is the y-axis measuring in the figure? Vaccinations per lifetime for a person born in that year…?
The Y access represents the number of inoculations in the routine childhood vaccination schedule up to age 6.
It never ceases to amaze me how many vaccinations we give our children. I always feel so bad for my son when we go in and he has to get like 5 shots at one time. I would be so pissed if my kid got autism cause my doctor messed up a routine shot.
If your child did have an adverse reaction, it would not be the Doctor’s ‘fault. You can’t ‘mess up a shot’. It all has to do with the child is pre-disposed to be damaged by the contents of the vaccine, which we do not know how to predict.
To be fair to the health care providers, when they give vaccines they are usually providing care at the standards that have been set by the federal government, their professional organizations, and their state legislatures. The rare serious adverse side effects from vaccines are usually caused by the vaccines themselves (either alone or in combination with some other factor), rather than because of some error by the health care providers.
That being said, the anger you can imagine yourself feeling is most certainly expressed by parents whose children they believe have been injured by vaccines (and some most likely were). It is hard not to empathize with anyone who has suffered a iatrogenic ailment (that is, an ailment caused by medicine or a medical provider).
I should read your book! But… What motivates cramming “as many as six vaccinations into one office visit”? Why the “rapid increase in the size of the vaccine schedule”? Are there practitioners administering alternative vaccine schedules that are just as effective but spread out over longer periods?
What motivates cramming “as many as six vaccinations into one office visit”?
Young children are typically only given their routine vaccinations during “well child” visits, which occur on regular intervals (typically 2-3 days after birth, and at months 1, 2, 4, 6, 9, 12, 18, 24, 30, then once every year after that). They typically do not receive vaccines when they are ill, so they usually don’t get shots when they are in the doctor’s office for illnesses. Most (about 25 of the about 35) inoculations occur in the first 18 months of life. So, doctors have 7 scheduled office visits to give children 25 inoculations. Months 2, 4, and 6 typically see the most inoculations.
Why so many, so soon?
It’s hard for most parents to point to any one of the vaccines given in the first two years of life and say “I’m not concerned about my child getting these illnesses…” The fact is that today’s routinely administered childhood vaccines are quite effective at reducing the incidence of the illnesses they target, so – when asked one at a time – which illnesses parents want to prevent, they seem willing to allow their children to be vaccinated against almost all of them. The exceptions to this are the chickenpox vaccine and Hep B, both of which seem to bother a large number of parents. For a short time beginning in 2006, the chickenpox vaccine was included in the MMR vaccine (making it the MMRV), but authorities withdrew recommendation of the combined vaccine in 2008 after data suggested that it increased the risk for febrile seizures.
Why the “rapid increase in the size of the vaccine schedule”?
Over the last 20 years we have had a wave of new vaccines that help prevent childhood illnesses. Take a look at the included chart. Most of the new vaccines help prevent communicable diseases that are especially problematic for children in daycare settings – among them are the hib, rotavirus, influenza, and pcv vaccines. The vaccines work well in preventing these illnesses, but since only about half of American children under the age of 3 are in daycare, many parents who don’t put their children in daycare consider these vaccines as unnecessary. Others, call them “convenience vaccines” because they prevent illnesses that are almost never life-threatening, so the claim is that the only reason they are used is to allow parents to avoid missed days at work because they had to stay home with a sick child.
Are there practitioners administering alternative vaccine schedules that are just as effective but spread out over longer periods?
Yes, a large number (some polls suggest as high as 40%) of parents who opt out of the routine schedule by adapting it in some way. The best known alternative schedule is offered by Robert Sears, and it is used by millions of parents. Vaccine advocates – like Paul Offit, for example – attack Sears’s schedule as dangerous because it keeps they youngest children vulnerable to vaccine-preventable illnesses. If her were pushed, I think he’d also admit that he also thinks that acceptance of Sears’s schedule is an admission that vaccine-anxious parents are justified in their fears. Offit is adamant that they are not justified in fearing vaccines and ought not be empowered to act on their (in his mind) unreasonable fears.
Thank You Mark! I so empathize with friends facing that decision and have one friend who falls squarely into the anti-vaccine camp. “Vaccine-anxious ” is a valuable term I hope becomes part of the discussion. I have one other question which may be a sensitive one. What would your personal approach to vaccinating your newborn be?
JohnH: Thank you for your kind words. I’m happy to hear that you find this useful.
Regarding your question about my personal approach to vaccinating a newborn: I fear you’ll find my answer unsatisfactory. Like all parents who have made conscious decisions about their children’s vaccinations – either to adopt, reject, or alter the required and recommended schedules – my wife and I have a plan for our children’s vaccines, and we have discussed that plan with our family doctor. That being said, I am not a physician, and I won’t dispense medical advice. Likewise, I don’t think that the decisions my wife and I made with our family doctor for our children’s vaccines would necessarily be appropriate for any other family. So, I have to beg out of providing any sort of explanation about the approach we’ve taken in vaccinating our children or general guidelines for vaccinating a newborn.
But, I will say this, decisions about childhood vaccinations are very important, both for the child and for the public’s health, and I would strongly encourage all parents to be thoughtful about the issue and seek good quality advice from accredited sources.
Thank You again Mark. I respect and appreciate your decision not to share the details, as indeed you point out, what’s right for you and your family may not be for everyone. I will be recommending your book to any expecting parents. I will be promoting the notion of ‘ vaccination anxiety’ and hope it finds its way into the mainstream discussion.
Well, this is a well-considered piece, that nonetheless points out to me that people who are “vaccine-anxious” do not seem to care – or know, perhaps? – about vaccines’ role in the history of public health. Where is the concern for their fellow humans?
And, I must say, the comment about “mercury-laden” thimerosol is rather unfortunate as well as vague. As a chemist, I certainly would not use wikipedia, but this entry includes the chemical structure. Thimerosal (or more correctly thiomersal) has one atom of mercury in its structure. I do not consider this “laden,” even though of course mercury is a serious neurotoxin. I think the phrase “mercury-containing” is more accurate.
http://en.wikipedia.org/wiki/Thiomersal
Wonderful Web site, Continue the excellent job. Thanks for your time!
It is perfect time to make some plans for the longer term
and it is time to be happy. I have learn this submit and if I
could I want to suggest you some attention-grabbing things or tips.
Perhaps you could write subsequent articles relating to this
article. I wish to learn more issues about it!
I think you have plenty of issues already. But yay! It’s happy time!
Vaccines are not single handedly responsible for autism but are a part of the reason. This is what the parents of an autistic child have proven in their book (Reducing Autism Poisoning Impacts. Author: Adeerus Ghayan). They have written in detail impacts of processed foods, bad air and most importantly vaccines on their autistic child. They were able to document each and every change in their son’s behavior and physical symptoms because they were giving their son farm fresh foods. They have abstained from giving sweets and unless necessary medicines. Their conclusion is: preservatives and chemicals in foods and environment are causing autism. This may be the only comprehensive study on impact of vaccines and processed foods and needs to be investigated in detail.
Given the mass accumulation of data that fails to show a causal relationship between MMR vaccines, vaccines containing thimerosal and other combination vaccines, it can be concluded that there is no need for parents to worry about vaccinating their kids. Multiple controlled and replicable studies performed worldwide cannot prove the link between autism and vaccination.
The talk of which “camp” you are in, makes it sound as though believing in one side or the other makes it true.
The truth is the truth, and people are more worried about the implications, no matter the consequences.
That is utter nonsense. See my comments under the Nature piece, vis á vis that tired “the truth is the truth” line. Wake up: that’s not science, it’s “I Fucking Love Science” pop cheerleading.