I just read Alexandra Stern’s fine new history of genetic counseling, Telling Genes (Johns Hopkins, 2012; $40 cloth/$25 paper/ $15 Kindle). Though Alex is my friend, I review her book here because her subject relates so closely to the themes of Genotopia. Alex and I played leapfrog around some of the same archives as we researched. Telling Genes and The Science of Human Perfection are complementary—and I mean that in the nicest possible way. With that warning of possible conflict of interest, I want to examine her history of genetic counseling with the same “critical and sympathetic” analysis (3) that she applies to the history of genetic counseling itself.
Like medical genetics, the history of genetic counseling is intimately bound to that of eugenics. And like medical geneticists, genetic counselors have been trying to shake off these eugenic associations for many years. Stern, though highly sympathetic to today’s genetic counselors, won’t let that historical firewall stand. Unflinchingly, she drives home the eugenic connections in every chapter.
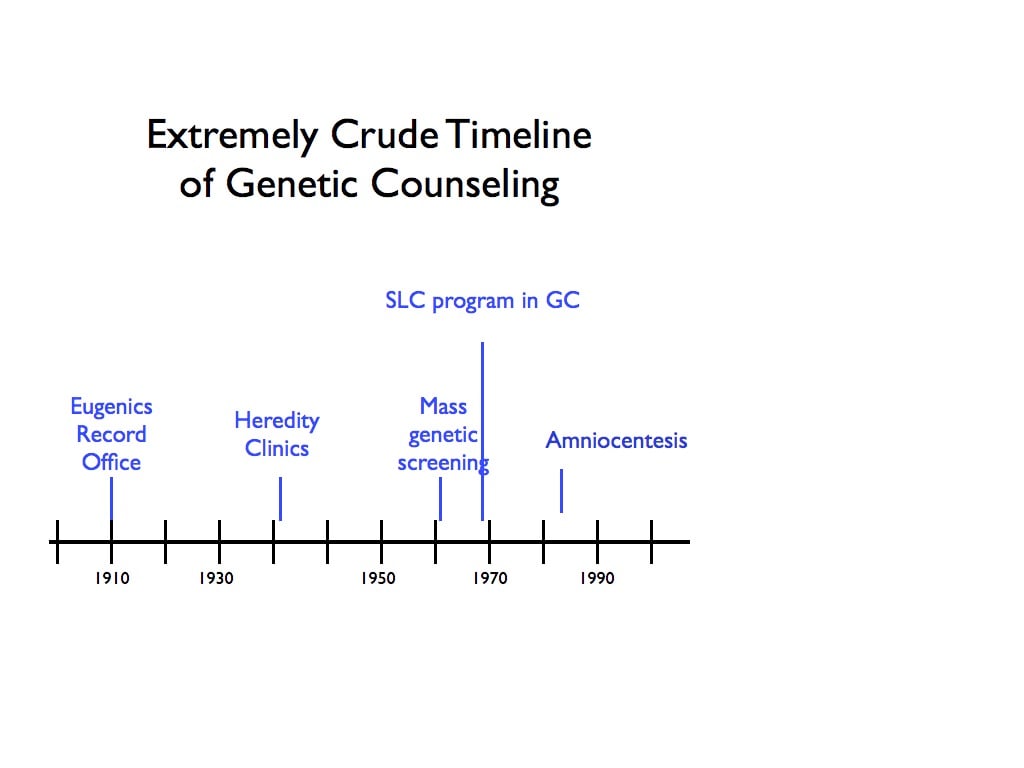
One of the most contentious issues in this history is where the history begins. Almost all genetic counselors today are Master’s level professional GCs. A Whig history of genetic counseling, then, might argue that the history began in 1969, with the founding of the first Master’s degree program in genetic counseling at Sarah Lawrence College. In contrast, a radical interested in showing the continuities with the darkest side of eugenics, might argue that the history began in 1910, with the founding of the Eugenics Record Office at Cold Spring Harbor. ERO staff advised people about many of the same things—likelihood of disease, of perpetuating family traits, of a particular racial parentage—that GCs still do today.
Stern takes a middle ground, beginning the history in 1941, with the founding of three independent research and counseling institutes for medical genetics: the Heredity Clinic in Ann Arbor, MI; the Family Record Office and Department of Medical Genetics at Wake Forest, and the Dight Institute of Human Genetics, in Minneapolis. These were conceived as Eugenics Record Offices attached to medical schools; collectively, they are known as the heredity clinics. At one of them (the Dight), the term “genetic counseling” was coined, by director Sheldon Reed, in 1947. Beginning here with these hybrid institutes—part ol’ time eugenics office, part modern genetic counseling facility— allows Stern considerable interpretive room. She allows the ambiguity and the tensions between individual and population to hang in the air, creating that kind of awkward pause in a conversation that makes a reflective person stop and think.
Stern does not, however, narrate the history chronologically. Rather, the history unfolds in a series of oscillations and resonances, in a series of analytic chapters organized by central concepts and problems in genetic counseling. Taking a thematic rather than chronological approach buys her a great deal of analytical substance, but it sacrifices narrative continuity. The arc of genetic counseling over the second half of the twentieth century doesn’t emerge until the end, and the reader must do the work of pulling out the major events and arranging them chronologically. Although the first chapter is titled “History,” it covers mainly the debate in the 1970s over the professionalization of the field. This is the only significant misstep in the book. A brief narrative account of the field—from the establishment of the Heredity Clinics in the early 1940s through the neo-eugenic 1950s, the emergence of genetic screening in the ‘60s, with the first Master’s level program at the end of the decade, through the profesionalization of the 70s and ‘80s, would have set the stage better for her later thematic analysis. I read the book with two graduate students, and both of them felt the lack of a chronological narrative to be a hindrance.
The remaining chapters cash in marvelously, often brilliantly, on the thematic organization. Chapter 2, “Genetic Risk,” looks at Huntington Disease, tracing the “shifting risk calculus” of the disease “as it crossed the transom of genetic testing and genetic counseling” (31). Stern notes that in lieu of effective therapies, more information and more precise diagnostics do not lessen—and perhaps increase—apprehension about the disease. Chapter 3, “Race,” focuses on questions of the population and the individual. Thinking in terms of populations, she argues, carries many tacit racial considerations into human genetics: “Population was never a neutral biogeographic term.” A harrowing and perceptive section on the methods of “racial matching” at the Dight Institute of Human Genetics in Minnesota and the Heredity Clinic in Michigan excavates a remarkable series of notebooks from the director, Sheldon C. Reed. Stern observes Reed simultaneously advocating publicly a liberal stance toward miscegenation as a solution to racial tension and advising adoptive parents on the goodness of fit of mixed-race children into a white family. Reed used an implicit “one drop rule,” At Michigan, James V. Neel—one of the pioneers of noneugenic medical genetics—also classified babies, according to a sort of Pantone series of skin tone. Stern allows this ambiguity to hang in the air, neither damning nor defending their inconsistency. These medical-genetic pioneers helped bring the field forward, but they were flawed, and Stern makes no apologies for them.
Chapter 4, on disability, focuses on the evolution of Mongolism to Down syndrome. In the 1940s, she shows, genetic counseling was built around a code of prevention (97). Gradually that code shifted to focus more on adaptation and adjustment, as families and patients’ rights groups have pressed for the acknowledgment of the disabled. These groups have understandably expressed concern over reproductive technologies and prenatal genetic screening, perceiving mandatory screening laws as an attack on the very existence of the disabled.
In chapter 5, “Women,” Stern relates the history of the founding of the Sarah Lawrence program in genetic counseling. Established in 1969 by Melissa Richter, it was brought to maturity by Joan Marks, who ran the program from Richter’s death in 1974 until 1998. Though mythologized as a moment when genetic counseling at last threw off its eugenic shackles, here too eugenic concerns mingle with sure-footed movements toward autonomy and informed consent. Richter, for all her sunny optimism and prescience, was a “neo-Malthusian,” couching her program proposal in the language of population explosion and mounting genetic “load,” Hermann J. Muller’s term for the accrual of mutations. Richter’s signal contribution was in establishing women as the foundation of modern genetic counseling—a startling echo (unnoted by Stern) of the long tradition of female “field workers” at the Cold Spring Harbor Eugenics Record Office in the teens and twenties. The medical community fought bitterly against the establishment of Master’s level genetic counseling, but the persistence of Richter and others persuaded physicians to cede jurisdiction over this critical but “softer” aspect of genetic medicine.
Chapter 6, on ethics, focuses on the shift from directive disease-centered eugenic counseling to nondirective, client-centered counseling. Here Stern takes us back to before the Heredity Clinics, to the psychologist Carl Rogers, who coined “nondirectiveness” in developing a new approach toward counseling victims of violence and abuse. She brings forward much fascinating and new material here, although her inference that Lee Dice and other Heredity Clinicians were borrowing directly from Rogers is circumstantial and, to me, not entirely persuasive. However, her analysis of the erosion of the concept of nondirectiveness is fascinating. She shows, surprisingly, that “nondirectiveness” has had a relatively short life. It didn’t enter the genetic counseling lexicon until the 1980s, and already by the 2000s it had begun to recede as the discipline’s gold standard, in favor of a more nuanced discussion about the strengths and limits of autonomy and consent.
The final chapter shifts categories to look at a recent methodological development: prenatal genetic diagnosis and its uneasy marriage with genetic counseling. This provides her with a vehicle for examining developments in genetic counseling since the 1970s. Her analysis of the rise of amniocentesis is a valuable contribution to literature by Rayna Rapp, Ruth Schwartz Cowan, and Robert Resta, among others. A conclusion briefly examines current-day practices and, in an original analytical move, closes by considering the possibility that the history of genetic counseling may be drawing to a close. As genomic medicine works to treat all disease as genetic in origin, the concept of genetic disease is gradually eroding. If genetics dissolves into biology, what exactly will genetic counselors counsel about? Stern closes with a call for genetic counselors to examine their history as a means of ensuring their future.
Yet if the juggernaut of geneticization continues unabated, there will always be a need for a medical-genetic middleman—or middle-person. Someone with serious genetic training but also skilled in psychology, ethics, and education. Someone whose time is not metered in quarter-hour increments (and billed in C-notes). Telling Genes is unflinching in tracing our hereditarian past, but sympathetic toward and highly supportive of those compassionate professionals who guide the rest of us into an ever more genetic future. It should be widely read, by genetic counselors, by clinicians, by future parents, and by anyone who is or knows someone who is affected by genetic disease.